Want to get involved? Click here to learn about internships, fundraising events, volunteering opportunities, and partnerships.
Our Helpline: 1-800-363-363
Want To DonateNATAL's Helpline 1-800-363-363
NATAL is an apolitical nonprofit organization that specializes in the field of war and terror related trauma. NATAL aims to advance the resiliency of Israeli society through treatment, prevention, public awareness and research.
Personal stories
“It was hard for me to return to myself after the war. I couldn’t understand how everyone just returned to normal as though nothing had happened. NATAL helped me to cope with what I had experienced, helping me to feel better one step at a time.”
“For years I lived with the pain of what I experienced until I saw NATAL’s ad and decided to call. From the first moment of contact you knew exactly how to help me. You know how to listen and helped me get the necessary treatment.”
“After the terror attack I felt extremely confused, shocked, scared and helpless. Calling the Helpline gave me support. You explained to me why I was reacting the way I was and were the only people I felt understood how I felt. Because of you I am on the path to healing.”
About us
Established in 1998, NATAL is an apolitical orgainzation that acts as a unique multidisciplinary trauma center aiming to treat those directly and indirectly affected by war and terror-related trauma in Israel. We aspire to lead the way in the field of trauma and to advance the resiliency of Israeli society through treatment, prevention, public awareness and research.

NATAL is a nonprofit organization. 100% of donations go in support of direct services and programs.
International Programs and Trainings
NATAL's expertise is sought by worldwide agencies including veterans organizations, academic and research institutions, government bodies and municipalities, first response and mental health professionals. With 20 years of practical in-the-field experience, NATAL offers a variety of international trauma trainings and emergency preparedness programs to various communities and professional groups around the world. Learn more by clicking on the icons below.
Emergency Preparedness and Crisis Intervention
Providing skills and tools in the leadership and management of emergencies and crises before, during, and after they occur.
Helping the Helpers
Trauma resiliency training for first response organizations, social workers, humanitarian aid and disaster relief professionals.
International Partnerships
Read about our past and current partnerships with organizations from around the world.
News
 This has been a challenging year for all, on a worldwide scale. The outbreak of COVID-19 has forced everyone to adapt to a new reality, and unfortunately it has also caused much pain and grief to so many. Since the outbreak of the virus, NATAL adapted its programs to cater also to those who are suffering from the stress, anxiety and grief that the pandemic is causing. We are proud to share with you our Annual Report for 2020 a The report offers a wide picture of NATAL's activities during the...
This has been a challenging year for all, on a worldwide scale. The outbreak of COVID-19 has forced everyone to adapt to a new reality, and unfortunately it has also caused much pain and grief to so many. Since the outbreak of the virus, NATAL adapted its programs to cater also to those who are suffering from the stress, anxiety and grief that the pandemic is causing. We are proud to share with you our Annual Report for 2020 a The report offers a wide picture of NATAL's activities during the... We invite you to enjoy our Supplement Haggadah including tips on resiliency and family activities, a fun addition to this year's Seder (created in collaboration between NATAL and the Masorti Movement.) Feel free to share with your family and friends abroad! Passover Supplement Haggadah
We invite you to enjoy our Supplement Haggadah including tips on resiliency and family activities, a fun addition to this year's Seder (created in collaboration between NATAL and the Masorti Movement.) Feel free to share with your family and friends abroad! Passover Supplement Haggadah- Medical teams in Israel are experiencing the severity of a crisis previously unbeknownst in the history of the country, at twice the volume of most other civilians. They are emotionally eroded, desperate, exhausted and experiencing multitudes of traumatic events without any time to digest them. At this point we all know that the Coronavirus is here to stay and that as such, medical teams are our most valuable asset in the fight against the pandemic. If we do not take care of them now, they will...
 Taken from Rami’s blog 24/11/20 *Trigger Warning: War, PTSD, * It is not easy being the child of a post-traumatic parent. It’s also not easy to be a father to your children when you suffer from post-trauma. I was blessed with 3 boys, and from the moment of their birth the dilemma of how I tell them arises. How am I meant to share my experiences of war? You want to tell them because it’s important that they recognize these aspects of who their father is, however at the same time there...
Taken from Rami’s blog 24/11/20 *Trigger Warning: War, PTSD, * It is not easy being the child of a post-traumatic parent. It’s also not easy to be a father to your children when you suffer from post-trauma. I was blessed with 3 boys, and from the moment of their birth the dilemma of how I tell them arises. How am I meant to share my experiences of war? You want to tell them because it’s important that they recognize these aspects of who their father is, however at the same time there... For the first time in Israel and in light of the growing need, we have established a new and specific Helpline to provide support and emotional assistance to first responders. The target population will include, paramedics, medical teams, nurses, doctors and social workers, who are required to "stand on the front line". First responders are required to cope with a heavy workload, exposure to difficult experiences, burnout and fatigue which now intensified during the outbreak of COVID-19....
For the first time in Israel and in light of the growing need, we have established a new and specific Helpline to provide support and emotional assistance to first responders. The target population will include, paramedics, medical teams, nurses, doctors and social workers, who are required to "stand on the front line". First responders are required to cope with a heavy workload, exposure to difficult experiences, burnout and fatigue which now intensified during the outbreak of COVID-19.... NATAL is proud to share the launch of a new podcast series, Empowering Responders: Helping Responders to Bend, Not Break. An extension of the UASI/NATAL Operational Stress Management (OSM) training program, these podcasts were developed to provide NJ first responders with guidance and coping techniques to manage the stressors they face in their professional lives. The podcasts were recorded by graduates of the OSM training program, medical experts, and leading professionals in the fields of...
NATAL is proud to share the launch of a new podcast series, Empowering Responders: Helping Responders to Bend, Not Break. An extension of the UASI/NATAL Operational Stress Management (OSM) training program, these podcasts were developed to provide NJ first responders with guidance and coping techniques to manage the stressors they face in their professional lives. The podcasts were recorded by graduates of the OSM training program, medical experts, and leading professionals in the fields of...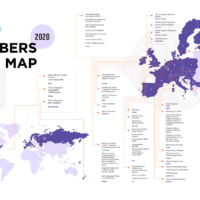 The #Covid19 pandemic has been spreading across the world and has a significant impact on our personal and professional lives. This pandemic summons the most primal human fears such as dying, loss of loved ones, isolation, loneliness, loss of control, and fear of the unknown. COVID-19 evokes complex and unique challenges for helplines, some familiar and some new. Today, most crisis helplines are stretched beyond their capacity due to surges in calls and limited manpower. Helplines must...
The #Covid19 pandemic has been spreading across the world and has a significant impact on our personal and professional lives. This pandemic summons the most primal human fears such as dying, loss of loved ones, isolation, loneliness, loss of control, and fear of the unknown. COVID-19 evokes complex and unique challenges for helplines, some familiar and some new. Today, most crisis helplines are stretched beyond their capacity due to surges in calls and limited manpower. Helplines must... Regardless of which side of the ocean we are on, we all feel stressed, anxious and fearful in light of the COVID-19 global pandemic and what the "new normal" will bring. NATAL is honored to have partnered and worked with communities around the globe, such as Chicago, to help provide tools and coping mechanisms to those suffering emotionally from COVID-19. NATAL is grateful to have such a long lasting and thriving partnership with JUF in Chicago and we are wishing everyone health, safety,...
Regardless of which side of the ocean we are on, we all feel stressed, anxious and fearful in light of the COVID-19 global pandemic and what the "new normal" will bring. NATAL is honored to have partnered and worked with communities around the globe, such as Chicago, to help provide tools and coping mechanisms to those suffering emotionally from COVID-19. NATAL is grateful to have such a long lasting and thriving partnership with JUF in Chicago and we are wishing everyone health, safety,... According to NATAL, since the COVID-19 outbreak, the Helpline has received approximately 6,000 calls • 40% of callers are 70 years old or older • Main concern: loneliness and helplessness. Noam Dvir Israel Hayom April 5th, 2020 More women than men are calling to receive help, and the elderly are more concerned. Ever since NATAL’s Helpline has opened to the general public to assist in coping with anxiety related to the COVID-19 outbreak, thousands of calls have been received. Two...
According to NATAL, since the COVID-19 outbreak, the Helpline has received approximately 6,000 calls • 40% of callers are 70 years old or older • Main concern: loneliness and helplessness. Noam Dvir Israel Hayom April 5th, 2020 More women than men are calling to receive help, and the elderly are more concerned. Ever since NATAL’s Helpline has opened to the general public to assist in coping with anxiety related to the COVID-19 outbreak, thousands of calls have been received. Two... NATAL has carried out various live video webinars for different populations and sectors who are dealing with emotional and psychological stress due to the Coronavirus. The webinars are an instrumental way to share guidelines and crucial tips to help the public remain calm and informed on best practices. Webinars are led by members of NATAL's Community Resilience Team who are experts in the field of emergency response, resilience, trauma, and dealing with stress....
NATAL has carried out various live video webinars for different populations and sectors who are dealing with emotional and psychological stress due to the Coronavirus. The webinars are an instrumental way to share guidelines and crucial tips to help the public remain calm and informed on best practices. Webinars are led by members of NATAL's Community Resilience Team who are experts in the field of emergency response, resilience, trauma, and dealing with stress.... Dear Friends, With the COVID-19 pandemic a global reality, this Peach brings new challenges to communities across the globe. For many this year, family Seder tables are replaced by computers, and the joy of the holiday is overshadowed by anxiety, isolation and uncertainty. NATAL's dedicated team of staff, clinicians and volunteers continue to work in Emergency Mode, finding innovative ways to bring support to those most in need, despite...
Dear Friends, With the COVID-19 pandemic a global reality, this Peach brings new challenges to communities across the globe. For many this year, family Seder tables are replaced by computers, and the joy of the holiday is overshadowed by anxiety, isolation and uncertainty. NATAL's dedicated team of staff, clinicians and volunteers continue to work in Emergency Mode, finding innovative ways to bring support to those most in need, despite... Despite it all: 10 ideas for a meaningful Seder Chat with parents about preparations throughout the day, include the kids, coordinate with extended family to hide the Afikoman in the same place, and get dressed up - without going anywhere. Family Seder - 2020. -Rakefet Ginsburg - For many families, the Passover Seder is a rare chance to gather everybody across the generations and all celebrate together. But this year, we have to keep it to a minimum. A few ways to cope with the new...
Despite it all: 10 ideas for a meaningful Seder Chat with parents about preparations throughout the day, include the kids, coordinate with extended family to hide the Afikoman in the same place, and get dressed up - without going anywhere. Family Seder - 2020. -Rakefet Ginsburg - For many families, the Passover Seder is a rare chance to gather everybody across the generations and all celebrate together. But this year, we have to keep it to a minimum. A few ways to cope with the new... As we all navigate the difficult circumstances brought on by COVID-19, NATAL has extended its services, offering additional support to those struggling with the anxiety related to the pandemic. NATAL is hosting a few webinars in the coming days. On Thursday we will be holding a webinar for parents led by members of NATAL's Community Resilience Team, experts in the field of emergency response, resilience, trauma and dealing with stress.. The webinar will be hosted in Hebrew for those of you...
As we all navigate the difficult circumstances brought on by COVID-19, NATAL has extended its services, offering additional support to those struggling with the anxiety related to the pandemic. NATAL is hosting a few webinars in the coming days. On Thursday we will be holding a webinar for parents led by members of NATAL's Community Resilience Team, experts in the field of emergency response, resilience, trauma and dealing with stress.. The webinar will be hosted in Hebrew for those of you... Maintain routine: Daily routine helps maintain a sense of security and stability. Maintain regular sleep, waking, studying and leisure time. When the whole family is quarantined you can set specific times for familial rituals such as meals and joint activities. Give each family member a role and share household chores. Stay informed: Information helps to enhance our sense of control. Stay up to date with the latest updates from the local ministries/agencies responsible for public health....
Maintain routine: Daily routine helps maintain a sense of security and stability. Maintain regular sleep, waking, studying and leisure time. When the whole family is quarantined you can set specific times for familial rituals such as meals and joint activities. Give each family member a role and share household chores. Stay informed: Information helps to enhance our sense of control. Stay up to date with the latest updates from the local ministries/agencies responsible for public health.... The spread of the Coronavirus is causing international alarm and worry, and we feel is our duty to respond to this current crisis. In light of this unfortunate pandemic, and as part of our understanding that this is a national crisis and emergency, NATAL's Helpline has extended its services to also support those suffering from anxiety and stress as a result of the spread of the virus in Israel and the uncertainty that it is causing. Just yesterday calls to our Helpline have risen by over 45%...
The spread of the Coronavirus is causing international alarm and worry, and we feel is our duty to respond to this current crisis. In light of this unfortunate pandemic, and as part of our understanding that this is a national crisis and emergency, NATAL's Helpline has extended its services to also support those suffering from anxiety and stress as a result of the spread of the virus in Israel and the uncertainty that it is causing. Just yesterday calls to our Helpline have risen by over 45%...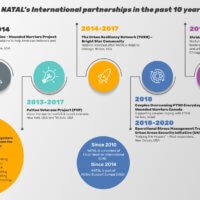 While NATAL’s work began in Israel, its mission resonates worldwide. In the past decade, NATAL has been called upon to deliver its deep expertise to at-risk communities and populations outside of Israel. As part of our recognition of the global need to support victims of trauma and to support communities in their quest to strengthen resilience we are happy to have led and participated in groundbreaking partnerships in a variety of service areas –working with US veterans dealing with...
While NATAL’s work began in Israel, its mission resonates worldwide. In the past decade, NATAL has been called upon to deliver its deep expertise to at-risk communities and populations outside of Israel. As part of our recognition of the global need to support victims of trauma and to support communities in their quest to strengthen resilience we are happy to have led and participated in groundbreaking partnerships in a variety of service areas –working with US veterans dealing with... This year's Annual Women's Event took place on the 4th of February, focusing on a panel of four women who live and work in the southern regions of Israel, unfortunately an area greatly affected by ongoing conflict. The panel included women working in the fields of mental health and education where who shared their personal stories on the reality of life in the south, and their need to remain optimistic and strong in order to overcome the many struggles they face. The panel included ▪ Adi...
This year's Annual Women's Event took place on the 4th of February, focusing on a panel of four women who live and work in the southern regions of Israel, unfortunately an area greatly affected by ongoing conflict. The panel included women working in the fields of mental health and education where who shared their personal stories on the reality of life in the south, and their need to remain optimistic and strong in order to overcome the many struggles they face. The panel included ▪ Adi... First responders are heroes to all of us! Standing in the forefront, saving lives, countless and never ending days of dedication and hard work. We at NATAL, are proud to Help the Helpers and to provide them with much needed psychological support to combat burnout and exhaustion, secondary traumatization and Post Traumatic Stress Disorder (PTSD). This year, NATAL took part in the IPRED International Conference on Preparedness & Response to Emergencies & Disasters (IPRED) to hear and...
First responders are heroes to all of us! Standing in the forefront, saving lives, countless and never ending days of dedication and hard work. We at NATAL, are proud to Help the Helpers and to provide them with much needed psychological support to combat burnout and exhaustion, secondary traumatization and Post Traumatic Stress Disorder (PTSD). This year, NATAL took part in the IPRED International Conference on Preparedness & Response to Emergencies & Disasters (IPRED) to hear and...- On January 31st a group of amazing and motivated people came together in Tel Aviv to raise money and awareness of NATAL, and to workout at Ido Lazan's BulletProof - Train For Life gym with the motto "We Train for Life". We are so grateful for the organizers, Rachelle Punski and Ido Lazan for this beautiful idea, and for everyone who came and was involved. Thank you!
 On February 27th NATAL took part in a touching ceremony to mark the opening of a new Youth Leadership Program that opened at the Meir Ort High School in Kiryat Gat, a town living under continuous rocket attacks in southern Israel. The ceremony, attended by the Inbar Foundation and family members, and the Kiryat Gat Municipality's department of Education included a touching film to commemorate the tragic loss of Inbar Attiya, who was killed in the terror attack at the Dizengoff Center, Tel...
On February 27th NATAL took part in a touching ceremony to mark the opening of a new Youth Leadership Program that opened at the Meir Ort High School in Kiryat Gat, a town living under continuous rocket attacks in southern Israel. The ceremony, attended by the Inbar Foundation and family members, and the Kiryat Gat Municipality's department of Education included a touching film to commemorate the tragic loss of Inbar Attiya, who was killed in the terror attack at the Dizengoff Center, Tel... As we approach Thanksgiving, NATAL would like to share what we are especially thankful for - YOU! On Friday we held our 7th annual "Running in Color" event including over 5,000 participants! It would not have been possible without all of your support and contributions. We would like to thank all those who ran, participated, and embraced this colorful event as we raised awareness for terror and war-related trauma in Israel. We would like to share our gratitude for the hundreds of volunteers...
As we approach Thanksgiving, NATAL would like to share what we are especially thankful for - YOU! On Friday we held our 7th annual "Running in Color" event including over 5,000 participants! It would not have been possible without all of your support and contributions. We would like to thank all those who ran, participated, and embraced this colorful event as we raised awareness for terror and war-related trauma in Israel. We would like to share our gratitude for the hundreds of volunteers... NATAL is honored to share that NATAL's Chairperson and Founder, Jude Yovel Recanati, and Executive Director, Orly Gal, took part in the 2019 IAC National Summit this past weekend in Miami! Jude was invited to participate in a very interesting panel discussing the role of philanthropy and elevating minority communities in Israel, including NATAL's special projects in strengthening the resiliency of Israeli minorities. It was an unforgettable and high-profile conference which brought together...
NATAL is honored to share that NATAL's Chairperson and Founder, Jude Yovel Recanati, and Executive Director, Orly Gal, took part in the 2019 IAC National Summit this past weekend in Miami! Jude was invited to participate in a very interesting panel discussing the role of philanthropy and elevating minority communities in Israel, including NATAL's special projects in strengthening the resiliency of Israeli minorities. It was an unforgettable and high-profile conference which brought together... Since the morning of November 12th, 2019, over 250 rockets have been launched into Israel, injuring 39 civilians and putting 5.5 million more in harm's way. Schools were closed across the country, keeping 1 million children at home. For some, the rockets bring trauma that is new and raw. For others, the...
Since the morning of November 12th, 2019, over 250 rockets have been launched into Israel, injuring 39 civilians and putting 5.5 million more in harm's way. Schools were closed across the country, keeping 1 million children at home. For some, the rockets bring trauma that is new and raw. For others, the... Supporting Your Children in Times of Stress In times of adversity and turmoil, stress evokes strong emotions and causes uncertainty in all of us. So what can you do to help children cope? Click on the PDF link below for a downloadable list of tips on how parents, caretakers and educators can help children cope. Supporting Your Children in Times of Stress
Supporting Your Children in Times of Stress In times of adversity and turmoil, stress evokes strong emotions and causes uncertainty in all of us. So what can you do to help children cope? Click on the PDF link below for a downloadable list of tips on how parents, caretakers and educators can help children cope. Supporting Your Children in Times of Stress- May 2018: NATAL in Emergency Mode It's been a complex few weeks at NATAL since the rise in hostilities. Over 700 rockets were launched into civilian populations with devastating results: countless residents of southern Israel were forced to stay home from work, spending most of these days taking shelter with their families. Schools were closed, affecting...
 Earlier this week NATAL Chair Ms. Judith Recanati and Director General Ms. Orly Gal wrote to the community in Pittsburgh Here is an excerpt from their letter Dear President Finkelstein, Mr. Orsini and everyone at the Pittsburgh Federation, "....On behalf of NATAL, please allow me to take this opportunity to express our deepest condolences for the tragedy that has befallen your community. We have been following the news out of Pittsburgh this weekend… needless to say, we are shocked and...
Earlier this week NATAL Chair Ms. Judith Recanati and Director General Ms. Orly Gal wrote to the community in Pittsburgh Here is an excerpt from their letter Dear President Finkelstein, Mr. Orsini and everyone at the Pittsburgh Federation, "....On behalf of NATAL, please allow me to take this opportunity to express our deepest condolences for the tragedy that has befallen your community. We have been following the news out of Pittsburgh this weekend… needless to say, we are shocked and... Follow the link to an interview with Judith Yovel Recanati published in the Lesley College Magazine about the establishment of NATAL. https://lesley.edu/stories/judith-yovel-recanati
Follow the link to an interview with Judith Yovel Recanati published in the Lesley College Magazine about the establishment of NATAL. https://lesley.edu/stories/judith-yovel-recanati 2018 is a special year for NATAL as it marks the organization's 20th year of operation since first opening its doors in 1998. When NATAL was founded, it included only the Helpline and Clinical Unit. Since that time it has grown exponentially in response to demand, serving the entire country through a range of trauma treatment and prevention services. In recognition of NATAL's contribution to Israeli society, a special ceremony was held at the residence of the Israel President, Reuvin Rivlin...
2018 is a special year for NATAL as it marks the organization's 20th year of operation since first opening its doors in 1998. When NATAL was founded, it included only the Helpline and Clinical Unit. Since that time it has grown exponentially in response to demand, serving the entire country through a range of trauma treatment and prevention services. In recognition of NATAL's contribution to Israeli society, a special ceremony was held at the residence of the Israel President, Reuvin Rivlin... 17 April 2018 Iyar 2, 5778 Innovative study provides the first real-time profile of trauma symptoms during protracted warfare An innovative study, conducted by the University of Haifa and NATAL – Israel Trauma and Resiliency Center, has provided the first real-time profile of trauma symptoms experienced by citizens on the front line during protracted warfare. The study, which was conducted during Israel’s Operation Protective Edge, found that people who reported having a startle...
17 April 2018 Iyar 2, 5778 Innovative study provides the first real-time profile of trauma symptoms during protracted warfare An innovative study, conducted by the University of Haifa and NATAL – Israel Trauma and Resiliency Center, has provided the first real-time profile of trauma symptoms experienced by citizens on the front line during protracted warfare. The study, which was conducted during Israel’s Operation Protective Edge, found that people who reported having a startle... Finding Healing in the Aftermath of Tragedy A Note from Parkland, Florida From NATAL Psychologist, Yotam Dagan March 2018 When crisis arises, whether due to natural or manmade disasters, NATAL professionals are often called upon to provide immediate assistance and early intervention techniques to those in the epicenter of trauma, often traveling as part of a delegation of experts with the Israeli Trauma Coalition. In the immediate aftermath of the school shooting at Marjory Stoneman...
Finding Healing in the Aftermath of Tragedy A Note from Parkland, Florida From NATAL Psychologist, Yotam Dagan March 2018 When crisis arises, whether due to natural or manmade disasters, NATAL professionals are often called upon to provide immediate assistance and early intervention techniques to those in the epicenter of trauma, often traveling as part of a delegation of experts with the Israeli Trauma Coalition. In the immediate aftermath of the school shooting at Marjory Stoneman... Every year NATAL is proud to take on a few volunteers who decide to spend their time in Israel learning about the organization and its mission. Read about Tamar's experience below. "This summer I had the privilege to come to Israel on an internship program and vied specifically for the chance to work at NATAL. The experience exceeded all expectation, as I gained work experience and created friendships in the heart of Tel Aviv. Throughout my internship I was encouraged to take...
Every year NATAL is proud to take on a few volunteers who decide to spend their time in Israel learning about the organization and its mission. Read about Tamar's experience below. "This summer I had the privilege to come to Israel on an internship program and vied specifically for the chance to work at NATAL. The experience exceeded all expectation, as I gained work experience and created friendships in the heart of Tel Aviv. Throughout my internship I was encouraged to take...
Contact Us
NATAL is here for you. Whether you are looking for support or require more information, we invite you to be in touch.